


Collateral Damage: Reversing the Trends of Pandemic-Triggered Mental Illness
By Lisa Rue, PhD., cliexa Senior Advisor Adolescent Behavioral Health
Findings from a 2021 study of cliexa’s holistic screening (cliexa-OPTIONS) for adolescents and young adults confirms early suspicions regarding mental health issues among adolescents and young adults. The collateral damage resulting from lockdowns during the Covid-19 national response has been devastating, with young people struggling to cope with a range of issues, including how to manage negative feelings of depression, along with anxiety and thoughts of suicide.
Independent research presented this month by Dr. William Merchant from the Department of Applied Statistics and Research Methods (ASRM) and Dr. Stephen Wright from the Department of Applied Psychology and Counselor Education (APCE) at the University of Northern Colorado found dramatic increases in the frequency of patients and clients (ages 14-24 years) dealing with a mental health challenge. The percentages are outlined in Figure 1.
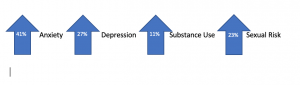
Figure 1. Percentages of UNC Students Exhibiting Various Mental Health Issues (N=202)
Parents and clinicians are facing difficulties in supporting these adolescents and young people. The continuum of mental health and wellness fluctuates regularly, increasing or decreasing depending on individual resiliency and support. While little can be done about individual genetic predisposition to depression or anxiety, certain measures can support young people by building resiliency or protective factors when increased risk is identified. Parents and clinicians can encourage resiliency and protective factors by asking a few targeted questions, such as:
Do you have a trusted adult, friend or family member that you can chat with? If not, can we think of someone together? Sometimes just being able to talk to someone about how you are feeling helps us cope.
Tell me some good things about yourself? What are some areas that you know you do well in that you can continue to develop? Let’s make a plan to spend more time building your skills and confidence in these areas.
Do you think people are respecting you? How do you think you can get people to respect your position and listen to your concerns? Sharing your concerns without getting angry will help communicate your concerns and validate
What makes you happy? What can you do to spend more time on things that make you happy?
What are some of your goals in the next 6 months? Two years? What are some steps you can take to meet those goals?
How has the pandemic affected your behavior and actions toward others? What can we control with respect to how we treat others during this difficult time?
A new resource available now, is the Dibble Institute’s new website for teens called Me and My Emotions (MeandMyEmotions.org), is a timely resource. Young people will find a wealth of information that they can use on their own to build resiliency, mindfulness skills, and improve mental wellness.
If mental health struggles sound familiar, remind your loved ones that they are not alone, and that life will eventually get back to normal. During this temporary struggle, it’s important to avoid using alcohol and other drugs to cope. Instead, focus on increasing your protective factors to decrease risks and create balance.
For more information about this study and its benefits, click here.

The power of remote patient monitoring
There is limited data comparing remote post-discharge patient treatment to that of standard in-person care, but a new clinical trial has done exactly that.
This multicenter randomized control trial measured safety events, medication adjustment and left ventricular reverse remodeling outcomes. The subjects were low-risk patients with acute myocardial infarction treated for 6 months after discharge by a centralized nurse practitioner–led telehealth program compared with standard in-person care by a cardiologist. There were no differences in achieved medication doses or indices of left ventricular remodeling.
This clinical trial set out to answer an important question for healthcare in a COVID and post-COVID landscape:
“Is remote post-discharge treatment of low-risk patients with acute myocardial infarction by a centralized nurse clinician team under physician supervision feasible and safe?”
The answer is: Absolutely. In fact, it’s both safe and effective.
What’s next?
Researchers now want to conduct a similar clinical trial with higher-risk patients, in an effort to further test the capabilities of remote intensive patient management and care. Read this impactful new study here:
The future is here:
cliexa-PULSE Home Health Monitoring Platform co-developed by cliexa and American College of Cardiology
“Imagine the ability to effectively capture RPM in the cardiology’s major disease states – HTN, CHF, CAD, and AFib in an easy-to-use-tool without all the data overload: Enter cliexa!” Dr. Andrew M. Freeman, MD – Director of Clinical Cardiology and Operations Director Cardiovascular Prevention & Wellness at National Jewish Health
Through the ACC Innovation Program with our partners at the American College of Cardiology (ACC), we have developed one of our latest modules, cliexa-PULSE to digitally transform and ultimately optimize cardiovascular care and outcomes. cliexa-PULSE is a mobile application designed for patients to track their symptoms, medications, episodes, complications and daily activity to manage Atrial Fibrillation providing real-time data to their clinicians. The expansion of cliexa-PULSE in 2021 will provide treatment tracking tools for patients with Hypertension, Congestive Heart Failure and Coronary Artery Disease, as well as launching a population health module. cliexa-PULSE is the ideal mobile app for clinicians to fully leverage patient-reported data, improving treatment decision-making and the overall patient experience. Learn more about cliexa-PULSE HERE
As of May 2020, we are proud to announce we have joined the StartUp Health Transformer Community. Joining over 325 global innovators in the healthcare space, StartUp Health organizes and invests in healthcare entrepreneurs in a worldwide community. As a leading healthcare venture fund, their unique approach to seed funding early-stage startups has established a diverse portfolio of entrepreneurs in all facets of health technology to achieve “moonshots.” These Health Moonshots aim to improve global healthcare, ranging from access to care to the ultimate goal of curing disease and cancer.
As their new portfolio company, we share their vision of tackling the access to care moonshot, as highlighted in the recent interview with our Founder & CEO, Mehmet Kazgan. StartUp Health allows cliexa to expand upon our Colorado reach to establish networks with other companies leading innovation in the healthcare industry nationwide. Our shared goal is to improve interoperability among each stakeholder in healthcare. Alongside StartUp Health, our digital screening, EMR integration, and remote monitoring paired with artificial intelligence (AI) will drive access to care regardless of patient’s demographics.
We are proud to join the global army of Health Transformers and are looking forward to the opportunities that will arise from this fruitful partnership.
Come check us out on our Company Profile for more information!

cliexa has been announced as a finalist for the 2020 Colorado Companies to Watch Award. We have been working diligently with medical providers, healthcare professionals, and expert technologists to improve patient care and treatment outcomes. Our platform has created notable impacts in healthcare through improved patient care, compliance, and technology use with predicting patient outcomes. As a finalist of the 2020 Colorado Companies to Watch Award, it is special to make a noticeable difference in our Colorado community.
Each year, Colorado Companies to Watch nominates Colorado-based businesses that rise to the challenge and help fuel the local economy. Since our inception in 2016, our goal is to make a difference in our community and have the ability to impact the future of healthcare.
2020 has brought a major turn of events for the local and national economies. We realize that 2020 will be a vital year for innovation and commitment in small businesses. Our team is dedicated to providing novel technologies that support the healthcare system. During this global pandemic, the cliexa team has worked to promote our Remote Patient Monitoring (RPM) and Telehealth services to healthcare systems around the nation. Our products provide a platform where healthcare providers can securely interact with their patients. It allows them to monitor patient activities and symptoms remotely to ensure continuity of care while shelter-in-place orders are active.
Innovative healthcare technology impacts more than just healthcare professionals; it affects everyone. cliexa creates solutions for patients, healthcare providers, and payors. Our team is proud to be a Finalist of the 2020 Colorado Companies to Watch Award, with a huge thank you to Bank of America for sponsoring this recognition!
In the past, cliexa has been announced by ColoradoBiz Magazine as a finalist at Prime Health Digital Challenge as well as Denver Metro Chamber 2020 Business Awards for Startup of the Year.